Together, we can positively impact patients living with alopecia areata
Alopecia areata (AA) is a chronic, complex, systemic, immune‑mediated disease characterized by sudden, non‑scarring hair loss on the scalp, face, and/or body. Beyond hair loss, patients often experience a significant psychosocial burden.
Learn more about AA and its impact below:
Disease Education
The better we understand AA, the better prepared we will all be in helping patients gain control over this disease.
TYPES OF ALOPECIA AREATA
Common Scalp Presentations

PATCHY AA
Patchy AA is characterized by ≥1 circular or oval patches that are smooth and devoid of hair. It can surface anywhere on the scalp and the size and number of patches may vary. Skin within the lesions is smooth, healthy-looking, and intact. Patients with patchy AA may experience spontaneous regrowth.1,2

ALOPECIA TOTALIS (AT)
Characterized by complete hair loss across the scalp, AT is a more advanced stage of the disease. AT can develop as an extension of patchy AA, or present as the initial manifestation. The absence of scalp hair is often permanent and increases the patient burden.2-4

ALOPECIA UNIVERSALIS (AU)
AU is characterized by the loss of all body hair, including the scalp, face, eyebrows, and eyelashes. AU is a severe form of AA.2,3
About 14%–25% of patchy AA cases progress to alopecia totalis or alopecia universalis.2,3
TYPES OF ALOPECIA AREATA
Uncommon Scalp Presentations

OPHIASIS PATTERN
Ophiasis pattern is characterized by hair loss in a band-like shape, extending across the occipital and temporal scalp.2,3

SISAIPHO PATTERN
Sisaipho pattern is characterized by a central hair loss pattern involving the frontal, temporal, and parietal scalp but sparing hair along the scalp periphery. It is also known as ophiasis inversus because the pattern is opposite to the ophiasis pattern and resembles androgenetic alopecia.2,3

DIFFUSE AA
Diffuse AA is rare and difficult to diagnose. Characterized by sudden, unexpected, non-patchy thinning of the hair all over the scalp. Diffuse AA is more common in female patients aged 20–40 years.2,3
Regrowth in one region of the scalp may be associated with expanding areas of alopecia elsewhere.3
TYPES OF ALOPECIA AREATA
Non-Scalp Presentations

EYEBROW AND EYELASH
Eyebrow and eyelash involvement is characterized with bilateral, patchy loss of eyebrow and/or eyelash hair. Eyelash involvement can affect both the upper and lower eyelids. Isolated eyelash involvement is rare; however, eyelash alopecia has been reported as a presenting sign of AA, particularly in severe cases.5

NAIL INVOLVEMENT
Nail involvement is characterized by distinctive pitting and roughening of the nail plate with longitudinal striations, or trachyonychia. It is more frequently associated with severe disease, such as AT or AU. Nail changes are observed in approximately 10%–15% of patients.2

BEARD OR BARBAE AA (BAA)
BAA represents a distinct subset of AA. It is characterized by well-circumscribed, round/oval patches that are smooth and devoid of hair mainly on the neck and jawline. Approximately 50% of cases will progress to extra-beard areas within 12 months. Beard involvement may be more noticeable in men with dark, coarse hair due to contrast with the underlying skin. Nail signs are notably absent in BAA.3,6
Eyebrow hair and eyelash loss can result in dryness and irritation in the eyes and an inability to keep debris or sweat from the eyes.1
THE EPIDEMIOLOGY OF ALOPECIA AREATA
Key Data and Demographics
The estimated prevalence of AA is 0.2%–2% of the population. AA affects females approximately 1.3x compared to males.1,7-9
An estimated 42% of AA patients have severe AA
as defined by the Severity of Alopecia Tool (SALT) score ≥50 and 58% have mild to moderate disease (SALT <50).7
Pediatric diagnoses represent approximately 20% of cases.10,11 Up to 40% of patients will present with their first AA patch before age 20.1,12
Non-white ethnicities have an increased risk of developing AA. Asian ethnicities have a 3x higher rate of AA compared with white ethnicities.13,14
BURDEN AND COMORBIDITIES
AA patients have a higher prevalence of immunological and psychiatric comorbidities7
The psychosocial burden in AA may be profound. Patients often face both public- and self-stigmatization.2,15-18
Up to 68% of patients with AA present with mental health symptoms. Diagnoses of anxiety and/or depression are more prevalent in AA vs age- and gender-matched controls.15,16
AA can significantly impact social and professional functioning and influence major life decisions.2,16
Increased risk of immune-mediated conditions in patients with AA vs controls without AA19
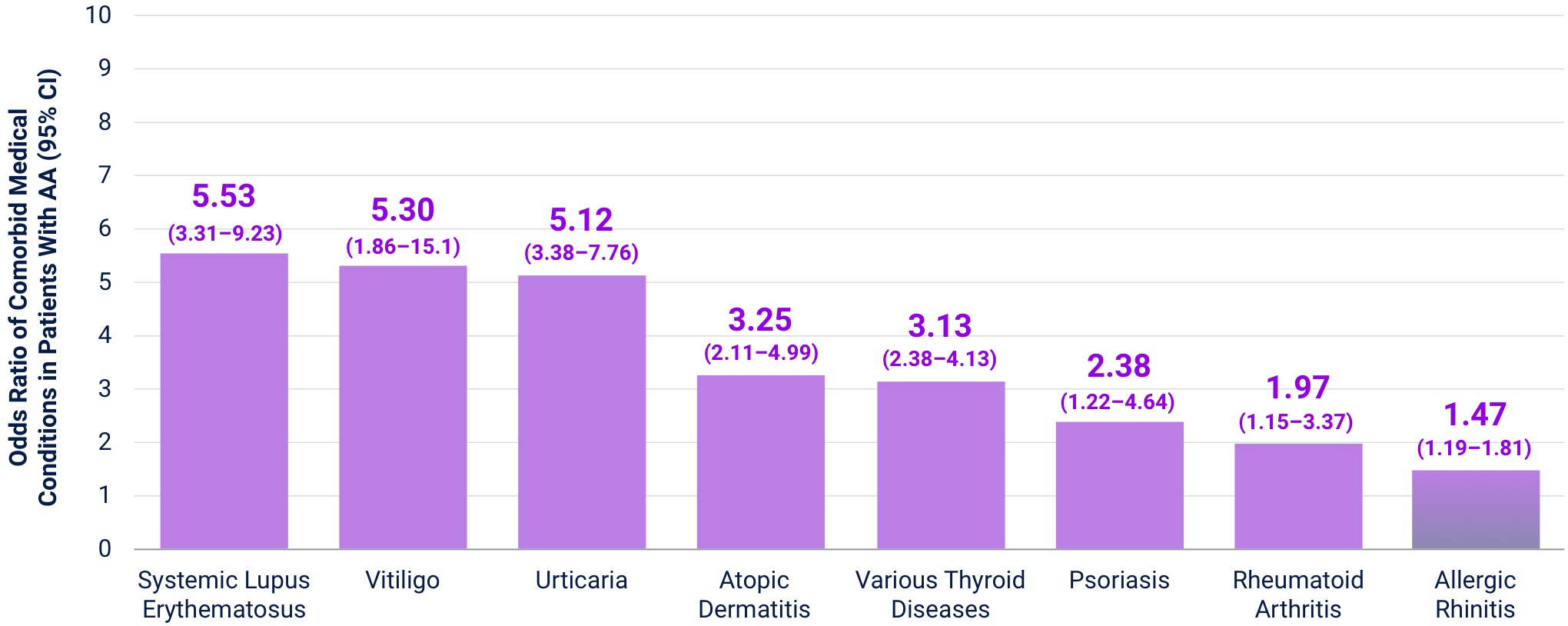
AA is associated with a 43% higher risk of new-onset atopic dermatitis (AD) and a 45% higher risk of other, new onset immune‑mediated conditions.19,20*
References: 1. Mesinkovska N et al. J Investig Dermatol Symp Proc. 2020;20(1):S62-S68. 2. Lepe K et al. Alopecia Areata. In:StatPearls;2024. 3. Pratt CH et al. Nat Rev Dis Primers. 2017;3(1):17011. 4. Lintzeri DA et al. J Dtsch Dermatol Ges. 2022;20(1):59-90. 5. Nguyen B et al. Am J Clin Dermatol. 2023;24(1):55-67. 6. Nwosu A, Miteva M. Skin Appendage Disord. 2023;9(3):179-186. 7. Benigno M et al. Clin Cos Inv Dermatol Clinical. 2020;13:259. 8. Mostaghimi A et al. JAMA Dermatol. 2023;159:411. 9. Villasante Fricke AM. Clin Cosmet Investig Dermatol. 2015;8:397. 10. Alkhalifah A et al. J Am Acad Dermatol. 2010;62(2):177-190. 11. O’Connor LF et al. Arch Dermatol Res. 2022;314(8):749-757. 12. Fricke AM. Clin Cos Inv Dermatol Clinical. 2015;8:397-403. 13. Harries M et al. Br J Dermatol. 2022;186(2):257-265. 14. Jang H et al. Eur J Clin Invest. 2023;53(6):e13958. 15. Ghanizadeh A et al. Int J Trichology. 2014;6(1):2-4. 16. Muntyanu A et al. J Eur Acad Dermatol Venereol. 2023;37:1490-1520. 17. Creadore A et al. JAMA Dermatol. 2021;157(4):392-398. 18. Kacar SD et al. Int J Trichology. 2016;8(3):135-140. 19. Ly S et al. Am J Clin Dermatol. 2023;24(6):875-893. 20. Holmes S et al. Clin Exp Dermatol. 2023;48(4):325-331.
Alopecia Areata Explained
You and your patients have many treatment options—such as topicals and systemic therapies—to consider for AA.
Take a look at information that may help with your treatment considerations.
UNDERSTANDING THE MECHANISM OF DISEASE
Watch how AA operates at a cellular level and learn what immune-mediated pathways can be targeted to help hair follicles return to a normal growth cycle.
Expert Exchange
Understanding AA and supporting patient-centric communications.

Making Each Moment Count: Meaningful Engagement With Our Patients

Goal Setting and Individualizing Targets With Our Patients

Understanding the Comprehensive Severity of AA for Patients

Helping Patients Navigate the Psychological Burden of AA

Tailoring Our Care: How Should Care Differ for Adult Patients vs Adolescents?
The Invisible Trauma of Alopecia Areata
Patient Stories
Watch these patient stories to gain a deeper understanding of how a life can be changed by AA.


