Severity of Alopecia Tool (SALT)
DESCRIPTION:
The Severity of Alopecia Tool (SALT) is a standardized method to quantify scalp hair loss in persons with alopecia areata (AA). Developed in the 1990s, SALT was formally adopted by the NAAF in 1999 and then revised in 2004.1-3 Often considered the gold standard for clinical trials, SALT allows clinicians and qualified HCPs to measure disease severity and track an individual’s response to treatment over time.2-4
DISEASE STATES:
Alopecia areata
VALIDATED USES:
Screening, severity assessment, treatment monitoring
ADMINISTRATION METHOD:
Clinician
COMMONLY USED IN:
Clinical trials, clinical practice
DETAILED DESCRIPTION:
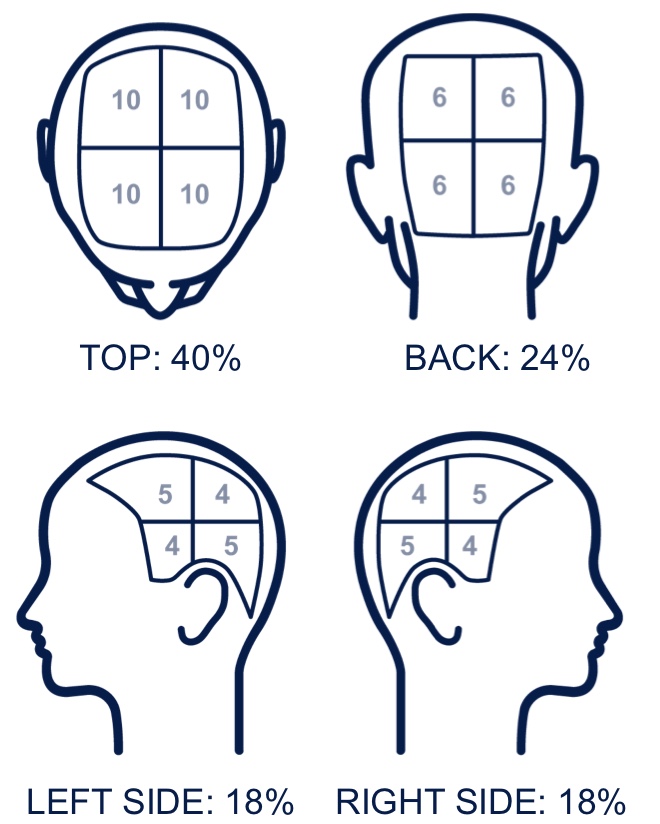
A SALT score relies on the determination of terminal hair loss or growth only. SALT is the main scoring system for percent scalp hair loss in AA clinical trials; it divides the scalp into 4 regions, or quadrants, with fixed weightings based on surface area: top (40%), back (24%), right profile (18%), left profile (18%). The clinician estimates the percentage of hair loss for each region and multiplies that number by its weighting factor, then sums all regions for a total SALT score. The sum of all regions results in a score that ranges from 0% to 100% (0=no scalp hair loss; 100=complete scalp hair loss).2,3 The assessment of disease severity is based on a 6-point subgroup classification or S bands (S0 to S5).1-3,6 Changes in the SALT score compared with baseline or the percent change from baseline may be used to track response to treatment in clinical trials.2 Clinical trials may use various SALT thresholds such as 50% and 90% improvement from baseline to define therapeutic success.7
In recent years, an Investigator Global Assessment tool (AA-IGA) has been developed. The AA-IGA uses SALT scores to describe therapeutic goals and severity bands. Key stakeholders aligned that a SALT score of ≤20% of scalp hair loss should be the therapeutic goal, and they also aligned on clinically meaningful gradations of severity. However, the AA-IGA based severity bands do not correspond exactly with the S bands that have been established in the original SALT development.6,7
VISUAL AID FOR ESTIMATING PERCENTAGE SCALP HAIR LOSS2
EXAMPLE: CALCULATING SALT2,3
SALT = Sum of scores for percent hair loss (range 0–100) x weighting factor for scalp region totals
| Scalp Region | Percent Hair Loss* | Weighting Factor | Scalp Region Totals |
|---|---|---|---|
| A. Top (vertex) | 0–100 x | 40% (0.4) | = 0–40 |
| B. Back (posterior) | 0–100 x | 24% (0.24) | = 0–24 |
| C. Right profile | 0–100 x | 18% (0.18) | = 0–18 |
| D. Left profile | 0–100 x | 18% (0.18) | = 0–18 |
| Total SALT score | = 0–100 | ||
*Note: In the above example, when estimating percent of scalp hair loss, use whole numbers, not decimals, and then multiply by the decimal weighting factor.
SALT SEVERITY: S BANDS1-3
| Severity Subclasses | Percent Hair Loss |
|---|---|
| S0 (no hair loss) | 0% |
| S1† | <25% |
| S2† | 25%–49% |
| S3† | 50%–74% |
| S4† | 75%–99% |
| S4a | 75%–95% |
| S4b | 96%–99% |
| S5 | 100% |
†This represents a revision of the S1–S4 categories from the original Alopecia Areata Investigational Guidelines.
AA-IGA BASED SALT SEVERITY BANDS7
| Score | Severity Subclasses | Percent Hair Loss |
|---|---|---|
| 0 | None | 0% |
| 1 | Limited | 1%–20% |
| 2 | Moderate | 21%–49% |
| 3 | Severe | 50%–94% |
| 4 | Very Severe | 95%–100% |
In 2016, SALT II was developed. Utilizing the “rule of nines,” SALT II assesses the percentage of scalp surface in smaller increments than what was established in the original SALT development. Essentially, SALT II further divides the 4 scalp regions (top, back, right, left) into smaller subunits that represent approximately 1% segments of scalp surface area.3-6 There is also a SALT adaptation for children called the Pediatric SALT score or pSALT. The pSALT score utilizes grids that are overlaid on head templates for specific age groups between 2–5, 6–11, and 12–21 years of age. However, over 11 years of age, the traditional SALT score has proven to be more accurate.4
VALIDITY:
The 1999 and 2004 SALT publications and the formal adoption by the NAAF guidelines suggest initial inter-rater reliability but lack statistical certanity.1,2 However, a 2024 publication, consisting of psychometric data, indirectly shows statistical inter-rater reliability. When replicating human-assigned SALT scores with AI, the AI systems demonstrated high intraclass correlation coefficients with human assessments (95% CI; ICC:0.97).8
LIMITATIONS:
SALT only measures scalp hair loss while ignoring body, eyebrow, and eyelash involvement, or other non-scalp measures. Because of this, some suggest it has low sensitivity and precision and underestimates the overall disease burden in AA.1-5 Also, the SALT
“S bands” lack clear descriptors for clinicians, thus introducing variability when assessing disease severity.6 The AA-IGA 5-point Likert-type scale severity bands attempts to standardize and reduce variability.7
CI=confidence interval; ICC=intraclass correlation coefficients; NAAF=National Alopecia Areata Foundation.
This resource is intended for educational purposes only and is intended for US healthcare professionals. Healthcare professionals should use independent medical judgment. All decisions regarding patient care must be handled by a healthcare professional and be made based on the unique needs of each patient.
References: 1. Olsen E, Hordinsky M, McDonald-Hull S, et al. Alopecia areata investigational assessment guidelines. National Alopecia Areata Foundation. J Am Acad Dermatol. 1999;40(2 Pt 1):242-246. doi:10.1016/s0190-9622(99)70195-7 2. Olsen EA, Hordinsky MK, Price VH, et al. National Alopecia Areata Foundation. Alopecia areata investigational assessment guidelines–Part II. National Alopecia Areata Foundation. J Am Acad Dermatol. 2004 Sep;51(3):440-447. doi: 10.1016/j.jaad.2003.09.032 3. Olsen EA, Roberts J, Sperling L, et al. Objective outcome measures: Collecting meaningful data on alopecia areata. J Am Acad Dermatol. 2018;79(3):470-478.e3. doi:10.1016/j.jaad.2017.10.048 4. Darchini-Maragheh E, Moussa A, Rees H, Jones L, Bokhari L, Sinclair R. Assessment of clinician-reported outcome measures for alopecia areata: a systematic scoping review. Clin Exp Dermatol. 2025;50(2):267-278. doi:10.1093/ced/llae320 5. Olsen EA, Canfield D. SALT II: A new take on the Severity of Alopecia Tool (SALT) for determining percentage scalp hair loss. J Am Acad Dermatol. 2016;75(6):1268-1270. doi:10.1016/j.jaad.2016.08.042 6. King BA, Senna MM, Ohyama M, et al. Defining severity in alopecia areata: current perspectives and a multidimensional framework. Dermatol Ther (Heidelb). 2022;12(4):825-834. doi:10.1007/s13555-022-00711-3 7. Wyrwich KW, Kitchen H, Knight S, et al. The Alopecia Areata Investigator Global Assessment scale: a measure for evaluating clinically meaningful success in clinical trials. Br J Dermatol. 2020;183(4):702-709. doi:10.1111/bjd.18883 8. Nguyen H, Gazeau L, Wolfe J. Using artificial intelligence to compute Severity of Alopecia Tool scores. JAAD Int. 2024;18:101-102. doi:10.1016/j.jdin.2024.04.003
Explore more clinical tools to improve dermatologic care for your patients.